The “UMFA”: Unmetabolized Folic Acid in Serum
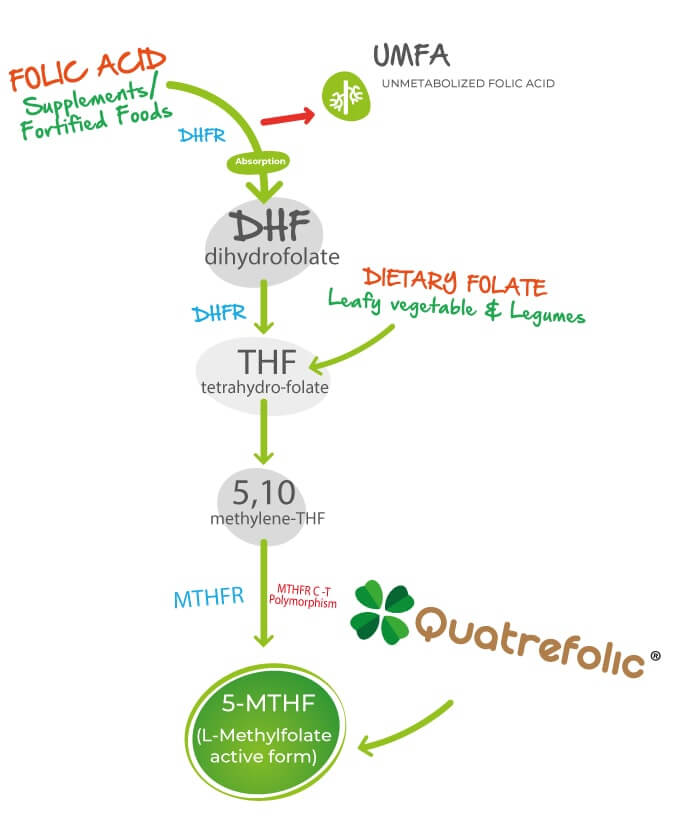
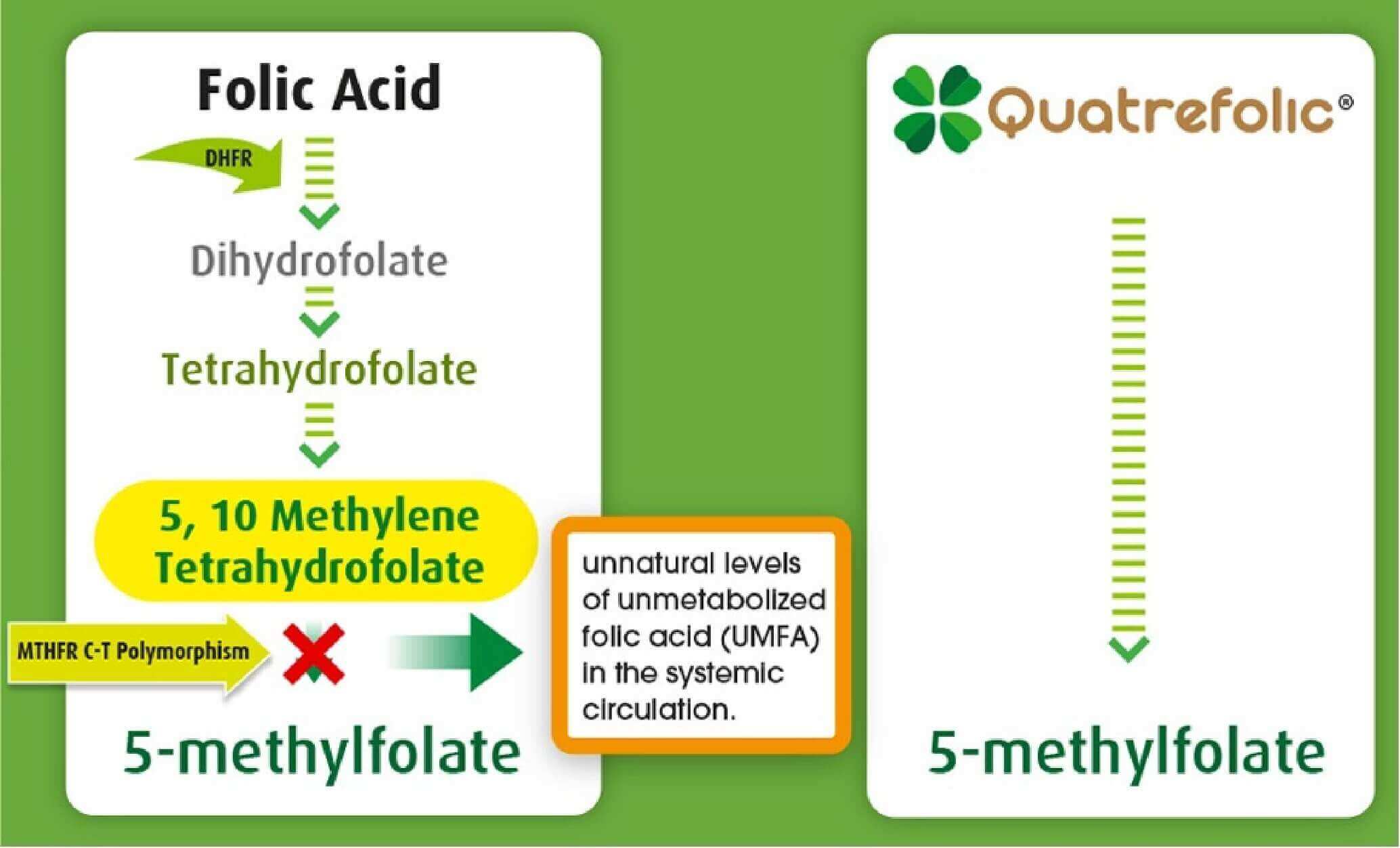
Since the implementation of folic acid fortification programs, several studies have reported increased circulating levels of unmetabolized folic acid (UMFA) in serum, raising questions regarding excessive intake and the body’s metabolic capacity to fully process synthetic folic acid [5–8]. Folic acid must undergo multiple enzymatic reduction steps, primarily through dihydrofolate reductase (DHFR), before conversion into the biologically active form, 5-methyltetrahydrofolate (5-MTHF). However, DHFR activity in humans is relatively limited and highly variable among individuals. When intake exceeds the body’s metabolic capacity, unmetabolized folic acid may accumulate in circulation as UMFA [13–15].
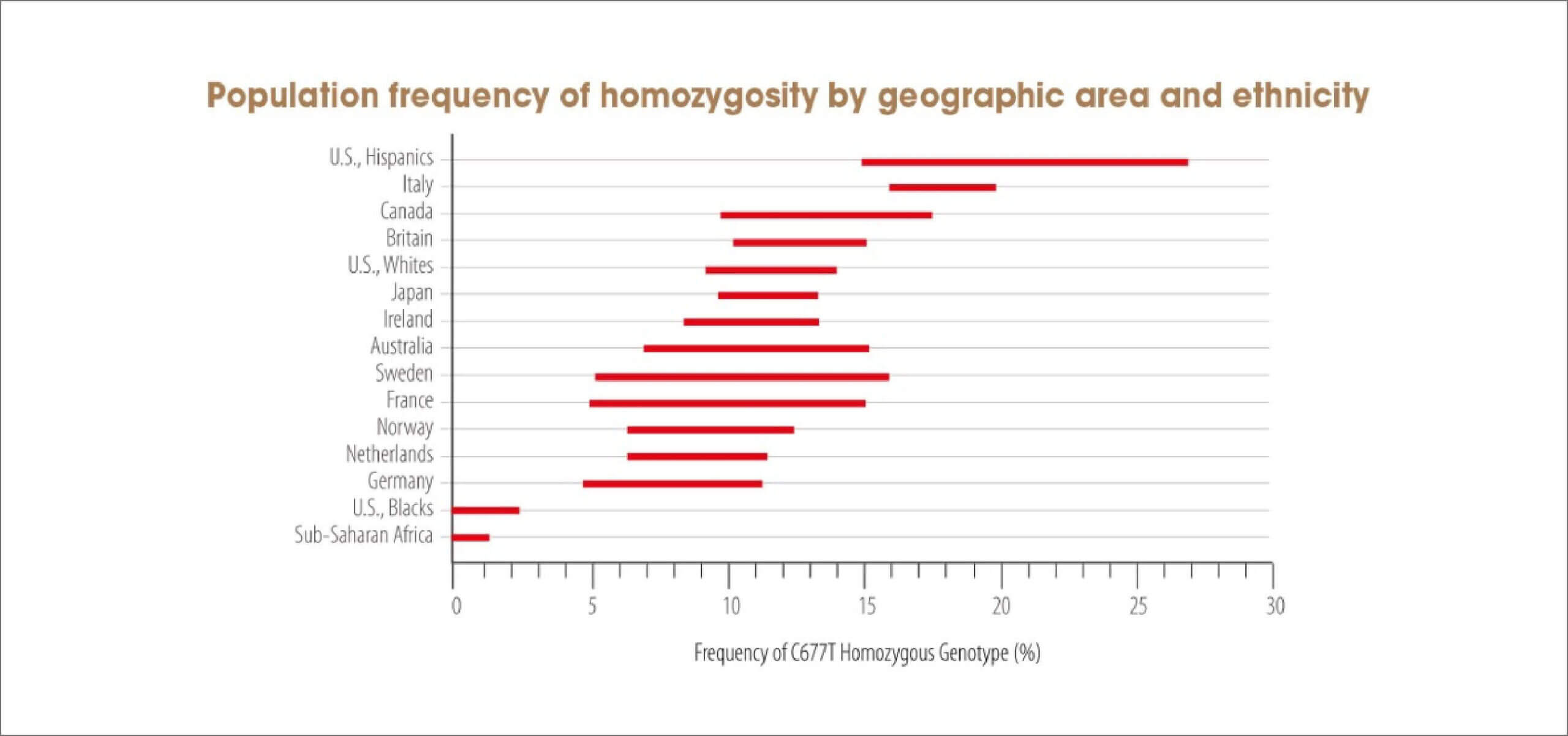
The persistence and variability of UMFA levels within the population may be influenced by several factors, including genetic polymorphisms affecting folate metabolism (such as MTHFR variants), impaired folate reduction pathways, liver dysfunction, chronic inflammation, and high intake from fortified foods and dietary supplements containing folic acid or folate [13–15].
Recent findings from the Frontiers in Nutrition study further demonstrated that supplementation with folic acid resulted in significantly higher serum UMFA concentrations compared with supplementation using 5-MTHF glucosamine salt. The study also observed a substantially greater proportion of individuals reaching supraphysiological folate concentrations in the folic acid group, while the 5-MTHF group maintained comparable folate status with markedly lower UMFA exposure [16]. These findings support the concept that active folate forms may provide more physiologic folate delivery while minimizing accumulation of unmetabolized folic acid.