News
Could Quatrefolic® be a complementary option in compromised bone health?
7 February 2022

The loss of bone mass, otherwise known as osteoporosis, mainly affects postmenopausal women due to a sharp decline in estrogen, but many other contributing factors, such as genetic and metabolic disorders, lifestyle, environmental and inflammatory factors, could play a role.
Modifiable risk factors have been identified as of paramount importance and are being heavily researched as they can be adjusted or changed to reduce the risk of disease development. Among them, elevated homocysteine (Hcy) serum levels may represent a risk factor for compromised bone health and skeletal fractures (1, 2, 3).
Little is known, however, about the mechanistic role of Hcy in bone health. At this time there is strong epidemiological evidence, that is being further reinforced by genetic studies, showing an association between the common MTHFR polymorphism and the risk of osteoporosis (3,4,5,6).
High levels of circulating Hcy have been shown in in-vitro studies to cause collagen cross-linking impairment, as well as impacting osteoclast and osteoblast activity, leading to poor bone health and fragility fractures (7).
The regulation of Hcy levels and the modulation of the inflammatory markers could represent additional therapeutic approaches not only for the protection of the cardiovascular system but also for bones, as suggested by recent research.
De Martinis et al. (1) has positively investigated the association between hyperhomocysteinemia and low bone mineral density (BMD). Hyperhomocysteinemia was also associated with high inflammatory marker C-reactive protein levels and low vitamin D, vitamin B12 and folate levels in 252 post-menopausal women.
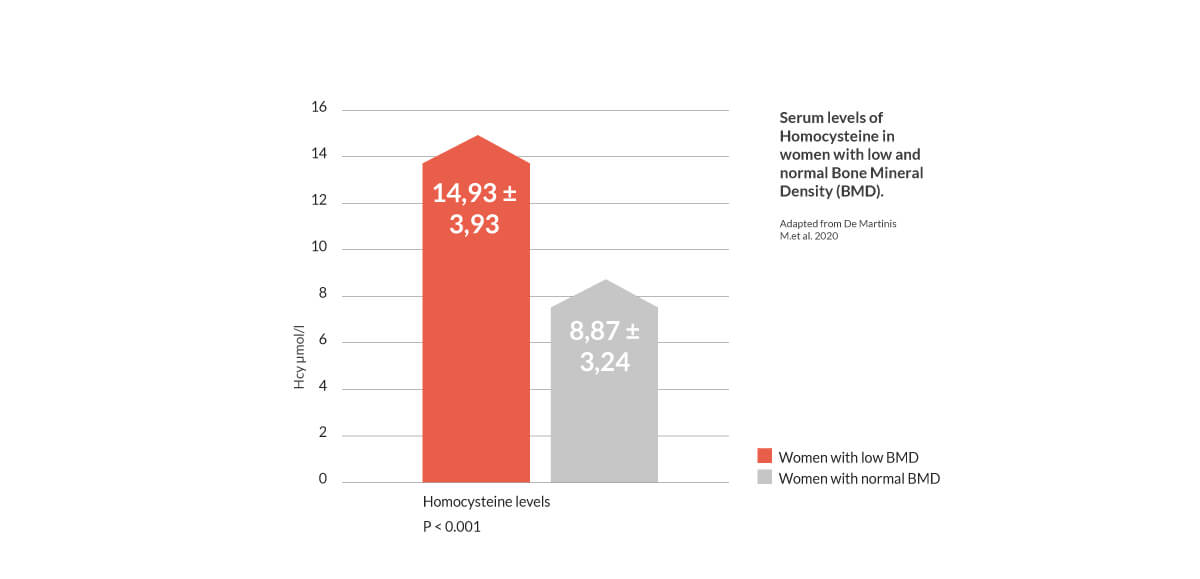
Hcy, inflammation, bone resorption markers, and prevalence of C677T polymorphism were higher, whereas vitamin D, B12, folate, and bone formation markers were lower in women with decreased BMD compared to those with normal BMD. Furthermore, 77% of women with low BMD presented with the C677T MTHFR polymorphism, while only 37% of women with normal BMD presented with the mutation.
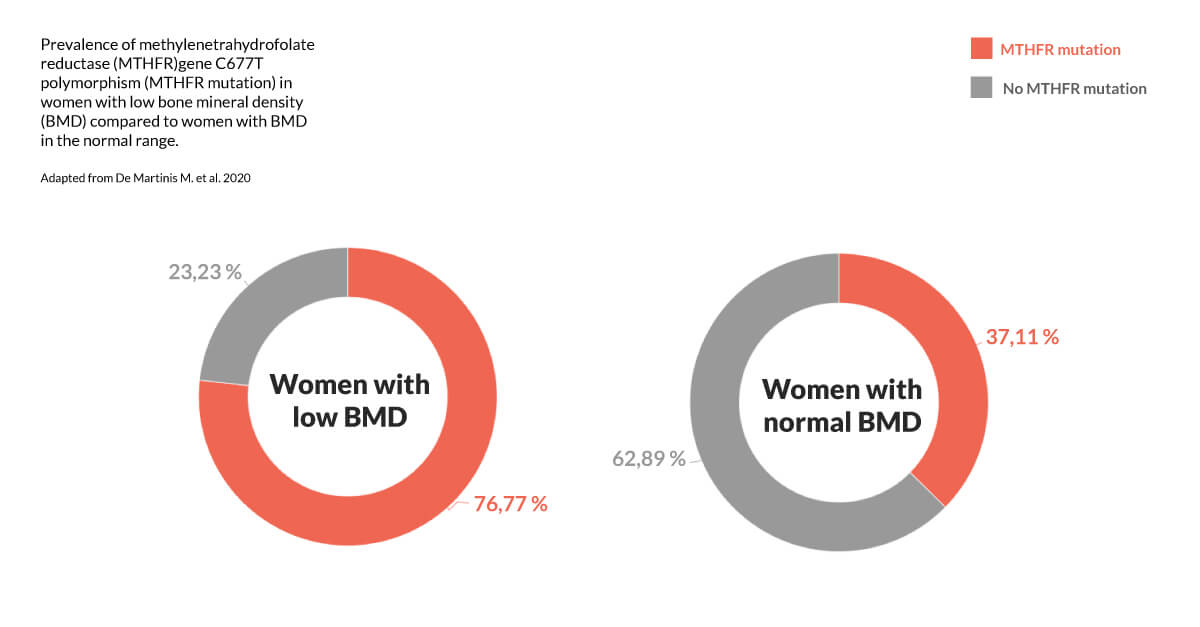
Taken together, these results suggest an association between the C677T MTHFR polymorphism and elevated Hcy levels and inflammation, which may further influence osteoporosis onset.
Quatrefolic® supplementation can help postmenopausal women to normalize Hcy, which contributes to bone health, and provides a form of folate that is biologically active and not dependent on the metabolization of the MTHFR enzyme.
Quatrefolic® has been shown to lower and normalize homocysteine levels in a randomized clinical trial where hypertensive subjects at low cardiovascular risk received 400 µg/day for 2 months versus a conventional vitamin supplementation with highly dosed folic acid (5 mg/day).
Quatrefolic® supplementation was more effective in reducing homocysteine serum level than folic acid, normalizing homocysteine in 55.8% of cases, significantly higher than in the control (8).
Observational and intervention trials have widely demonstrated that Vitamin K2 in the form of menaquinone-7 (MK-7) is a vital nutrient for supporting bone health. Vitamin K2 as MK-7 is required for the activation/carboxylation of a specific protein – osteocalcin – which is one of the most abundant proteins in bone, synthetized by osteoblasts.
Since first reported, carboxylated osteocalcin (c-OC) levels were correlated with and have been used as a specific marker for bone formation. c-OC has a higher affinity for calcium and thus stimulates the formation of hydroxyapatite and bone mineralization. A meta-analysis published in 2015 showed that vitamin K2 as MK-7 plays a role in osteoporosis in postmenopausal women. Nineteen randomized controlled trials were included in the analysis. Subgroup analysis of postmenopausal women with osteoporosis revealed a significant improvement of vertebral BMD for both medium- and long-term results, favoring the Vitamin K2 group. There was a significant reduction in undercarboxylated osteocalcin while there was an osteocalcin increment (9).
In 2013, Knapen et al. showed that a daily nutritional dose of MK-7 (180 mcg as MenaQ7®) for three years demonstrated for the first time clinically statistically significant protection of the vertebra and the hip (femoral neck) against bone loss. In this study of 244 healthy post-menopausal women, the MenaQ7® group showed significantly decreased circulating uncarboxylated osteocalcin (ucOC), a well-established biomarker for bone and vitamin K status. After 3 years, both bone mineral content and bone mineral density, as well as bone strength, were statistically significantly better for the MK-7 group compared to the placebo group. (10).
The postmenopausal period of women’s lives exposes them to important changes in bone structure, increasing their risk of osteoporosis, one of the main causes of disability and mortality in the elderly (1). It is an age-related skeletal disease characterized by decreased bone mineral density (BMD) and bone structure deterioration resulting in an increased risk of fractures. The combination of Quatrefolic® with Vitamin K2 as MK-7, such as MenaQ7® or vitaMK7®, could be interesting and innovative to promote and protect women’s bone health. While the active folate Quatrefolic® can contribute to their health through regulating and controlling healthy levels of Hcy, Vitamin K2 as MK-7 works to increase bone mineral density and promotes bone quality, protecting bone structure and metabolism associated. In this light Gnosis by Lesaffre is proud to highlight the great opportunity to combine its Quatrefolic® brand with its MenaQ7® or vitaMK7® K2 brands to innovate the bone health market, providing advantages for its partners.
REFERENCES:




